“I’ll think about it and get back to you.” Said politely, with a smile, on the way out the door. For any practitioner who has walked a patient through a full facial harmonization plan — areas, products, expected outcomes — that phrase lands harder than it looks.
It is almost never a rejection. It is uncertainty. The patient heard the protocol in clinical language, nodded along, and probably wants the result. But they cannot picture their own face after the treatment — and people do not commit to what they cannot see.
This is the gap that a facial harmonization simulator is designed to close: not through persuasion, but through clinical visual communication.
The Invisible Wall Between Interest and Decision
There is a well-documented pattern in aesthetic medicine consultations: patients who are interested in a procedure but leave without committing share a consistent profile. They are not skeptical of the practitioner’s skill. They are not opposed to the investment. What they lack is a personalized, concrete visual reference for the outcome.
Generic before-and-after galleries, however impressive, carry an implicit disclaimer the patient feels even if they do not say it aloud: “But that’s not my face.” Every face is unique, every concern has a personalized answer — and when the consultation relies only on verbal explanation and third-party imagery, the patient defaults to the one cognitive shortcut available: time. They will go home, research, ask people they trust, perhaps consult another clinic.
“I’ll think about it” is the behavioral signature of a patient who needed to see and didn’t.
What the Science of Visual Decision-Making Tells Us
Research in clinical communication consistently shows that patients decide faster and with greater confidence when they can project the outcome onto their own face — not onto someone who looks like them. This holds across dental aesthetics, reconstructive procedures, and facial harmonization.
Behavioral scientists call it identification with the outcome. The moment a patient sees a projection built from their own photograph, they stop evaluating an abstract service and start evaluating a future version of themselves. The internal question shifts from “Will this work for someone like me?” to “How soon can I do this?” — which is the natural consequence of replacing abstraction with visual evidence.
Clinical Simulator vs. Consumer Filter: Why the Distinction Matters
A clinical facial harmonization simulator is not a social media filter. Consumer apps apply cartoon-level changes that flatten features, erase texture, and produce projections that look nothing like what an evidence-based protocol actually delivers — leaving patients with unrealistic expectations before the conversation even starts.
A clinical tool works from a standardized photo taken in the office. It reflects the practitioner’s defined protocol — areas, products, real dosages — and generates a projection that preserves the patient’s identity rather than replacing it. The output is designed to inform a clinical decision, not to impress on a screen.
A Guided Consultation Sequence That Works
Integrating a facial harmonization simulator into a structured consultation follows a logical clinical sequence rather than a separate demonstration step. A typical flow looks like this:
- Standardized photograph: captured in-office under consistent lighting — the reliable baseline for analysis, simulation, and future comparison.
- Protocol definition: the practitioner selects treatment areas, products, and real dosages as part of the clinical plan, before the simulation runs.
- AI-generated projection: a personalized visual result built from the patient’s own image, reflecting the defined protocol.
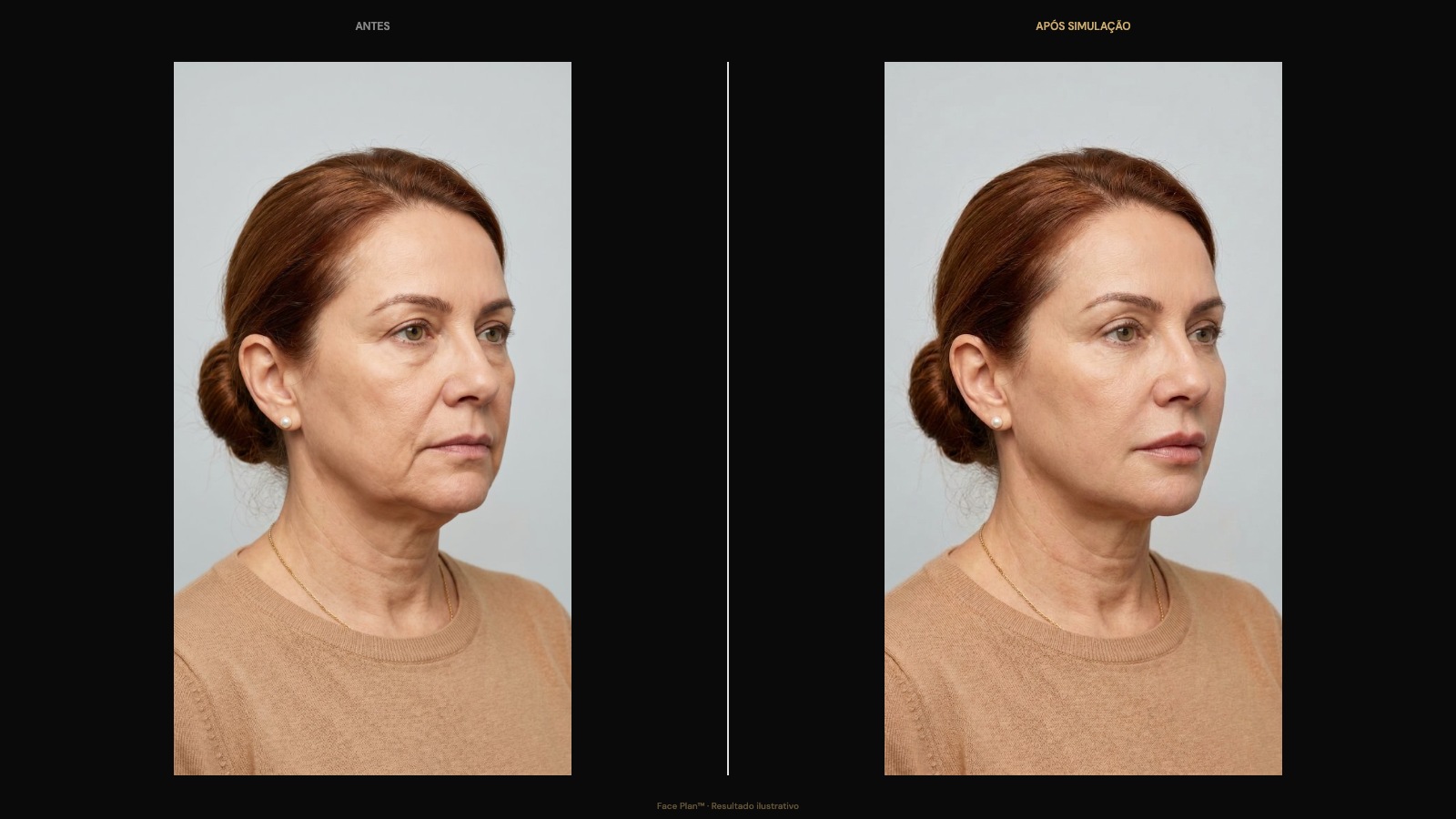
- Side-by-side comparison: before and after displayed simultaneously on screen, giving the patient a clear, objective visual reference.
- Clinical report and dual treatment plan: a structured document with protocol details, areas, dosages, and orientation for the patient to keep.
- WhatsApp video: a comparison video ready to send to the patient immediately, extending the visual experience beyond the appointment.
The entire sequence happens within the consultation time, without external software dependencies or manual post-processing. The practitioner leads the clinical conversation; the simulator translates the plan into a visual patients can respond to.
What Actually Changes When Patients See Their Face First
The immediate effect — a higher rate of same-session decisions — is the most visible outcome. But the clinical impact runs deeper than consultation conversion. When patients see a projected result before the procedure, three things shift in the clinical relationship:
Expectation alignment: the patient has a concrete visual reference before treatment begins. This dramatically reduces the post-procedure frustrations that come from mismatched expectations — the gap between what the patient imagined and what “natural enhancement” actually means for their specific face.
Richer informed consent: the simulation reinforces the verbal explanation and the consent document. When patients can see and discuss the treatment visually, their understanding is deeper and more durable.
Long-term retention: patients who go through a visually structured consultation report a higher perceived quality of care. They refer people in their network and return for maintenance with less friction. The consultation becomes the start of a lasting clinical relationship.
Practitioners affiliated with Full Face Academy have access to Face Plan™, the clinical simulator built specifically for in-office facial harmonization — with a guided consultation flow, real dosages, a structured clinical report, and a dual treatment plan on the same screen. If you want to understand how this technology fits your practice and what the consultation sequence looks like in a real clinical setting, explore the method and see how other practitioners are using patient visualization as a genuine clinical differentiator.
Disclaimer: Simulations generated by Face Plan™ are intended for educational and clinical communication purposes. They do not constitute a medical diagnosis or a guarantee of aesthetic outcome. Actual results depend on individual patient factors, practitioner technique, and clinical conditions.

